Wouldn’t it be nice to be able to time travel back and just properly isolate the various patient zeroes from the current outbreak?
So, first up – here is the latest news on the current outbreak.
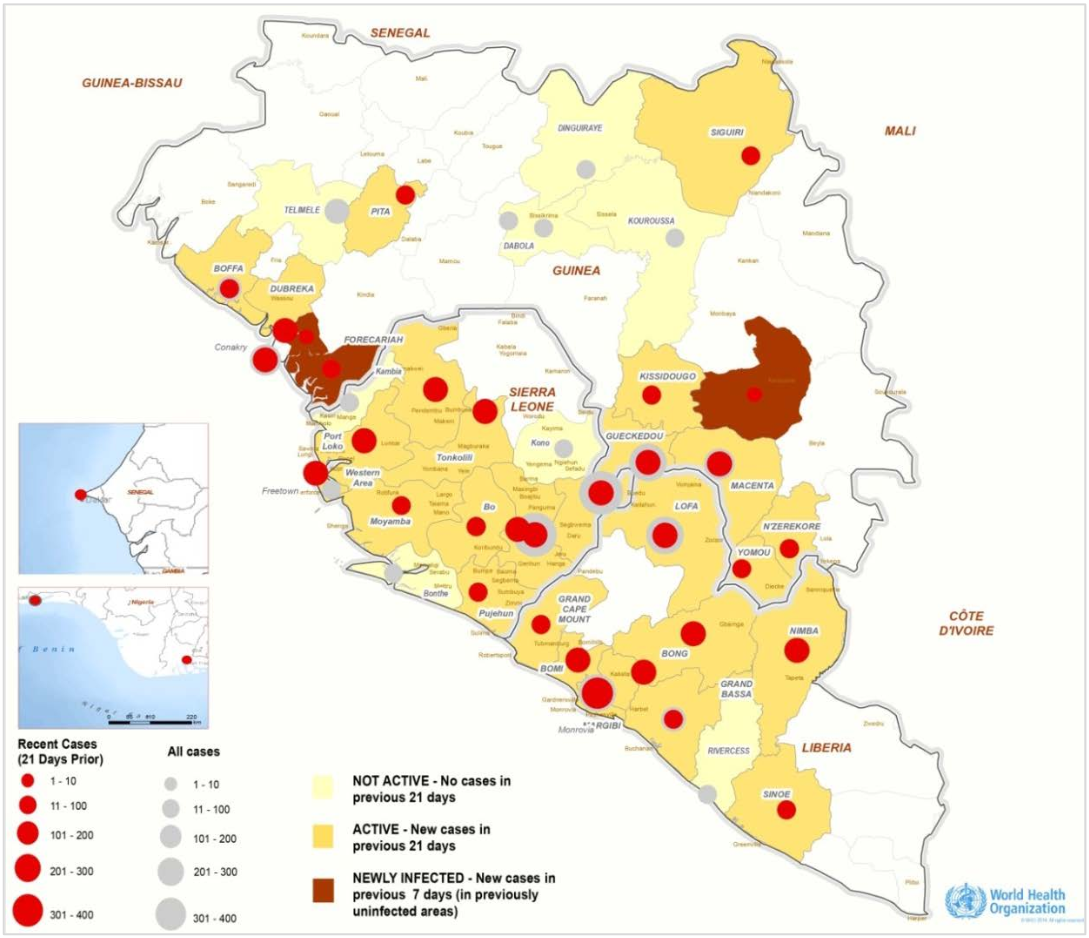
First up, the number of infected, and the number of fatalities in the West Africa outbreak was 3685, with 1841 deaths, as at 31 August. These data, along with the following picture are taken from the September 5 World Health Organisation (WHO) situation report.
http://www.who.int/csr/disease/ebola/situation-reports/en/
Below is a link to the WHO roadmap for scaling up international response to the outbreak. Important point – this roadmap is designed to stop transmission in infected countries within 6-9 months, and to prevent international spread.
One interesting point is, at the date of publication, 40% of infections had occurred within the previous three weeks.
http://www.who.int/mediacentre/news/statements/2014/ebola-roadmap/en/
All in all, the picture of an outbreak with the ability to explode past an epidemic into a pandemic if handled incorrectly. Thankfully, the strains involved have shown no propensity for aerosol spread so infection containment procedures are relatively simple.
Current containment protocols have somewhat limited the spread of disease, with more than 80% of cases occurring in 9 out of the 42 districts in Guinea, Liberia, and Sierra Leone that have reported cases (Lofa, Kailahun, Kenema, Gueckedou, Montserrado, Macenta, Conakry, Margibi, and Nimba).
The aid workers, doctors and various healthcare professionals involved will be facing an uphill battle unfortunately. Cultural response to must be managed to limit spread of disease, and although WHO has mandated that increased social mobilisation and community engagement is to be one of the cornerstones of their containment strategy, there is always the possibility of said communities not cooperating.
Really, what’s more to be said? A response is being applied, and only time will tell whether more drastic measures need to be taken. I must admit that epidemiology was never one of my favourite subjects.
Recent advances in the treatment of Ebola
Currently, the most successful treatment for Ebola is ZMapp, with a 71.5% success rate. Something to note though is that the current outbreak has an ~53% lethality, so it’s difficult to get a good picture of how effective ZMapp is. Granted, it’s more than a little heartless to do a proper randomised double-blind test on the efficacy of Ebola treatments, don’t you think?
Currently there are three additional treatments that have been shortlisted (Favipiravir, TKM-Ebola and BCX4430) and two vaccinations (NAID/GSK and VSV-EBOV). Testing has shown that the majority of these protect monkeys and mice from Ebola.

Another target for future Ebola treatments is development of compounds that will selectively block the entry of Ebola virus into host cells by disrupting the interaction between Ebolavirus spike glycoprotein (GP) and the endo/lysosomal cholesterol transporter protein Niemann–Pick C1 (NPC1). Tests performed in 2011 showed that cells deficient in the NPC1 protein were protected against infection against Ebola.1
For further reading, the following two links to Nature articles are some additional commentary on the current outbreak and what can be done to help treat/contain it.
http://www.nature.com/news/largest-ever-ebola-outbreak-is-not-a-global-threat-1.15640
http://www.nature.com/news/should-experimental-drugs-be-used-in-the-ebola-outbreak-1.15698
Stay angry my friends.
1: Côté M, Misasi J, Ren T, Bruchez A, Lee K, Filone CM, Hensley L, Li Q, Ory D, Chandran K, Cunningham J. 2011. Small molecule inhibitors reveal Niemann-Pick C1 is essential for Ebola virus infection. Nature. 2011 Aug 24;477(7364):344-8

Hello,
I really enjoyed reading your blog about Ebola. I’ve been pouring over the databases trying to learn more about this recently, and yours was a well-researched, well-organized perspective. My main reason for scouring the internet stemmed from the WHO’s “Chronology of previous Ebola virus disease outbreaks” http://www.who.int/mediacentre/factsheets/fs103/en/
It seems odd to me that there are no reported cases between 1979-1994. It seems even more odd that there is no mention of WHY it disappeared for 15 years. Maybe the reason is so glaringly obvious to everyone else that they don’t feel the need to state it…but it’s not obvious to me, and I’m surprised that this isn’t a question that more people are asking. (I did try to contact the WHO about this and received an auto-response stating that they don’t respond to requests from students.)
I suspect that the lack of reported cases is related to cases not being reported, rather than cases not existing. I’ve found this article, discussing how relations between the different health associations were affected by apartheid in South Africa, specifically from 1979-1994.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4006146/
I’m curious to know if this is something you have noticed or looked into? How would you explain the gap?
Thank you very much!
Kat S
Hi Kat,
First of all, thanks for the encouraging comment! Very nice to know I did a good job with my posts.
It’s interesting to note that the WHO timeline doesn’t note the Reston Ebola outbreak, which happened in 1989 (a fact that I forgot to mention in part one, whoops!), or any outbreaks in research animal colonies. On one hand, this shortens it to a 10-year gap in reports, on the other, it’s still a 10-year gap.
Personally, I think that it was actually the case that there were no cases to report. At the time, Ebola was so entrenched in the national consciousness of the African countries that it would be very unlikely that even a single case would not have gone unreported, as you can see with the table you posted, with single cases reported in Cote d’Ivoire and the Democratic Republic of Congo. Also, if you look at the species of Ebolavirus implicated in the different outbreaks, you can see that the Zaire strain was implicated in the 1994 Gabon outbreak, and the 1977 Democratic Republic of Congo case. Geographically speaking, these two countries are very close to one another, so the same viral reservoir could have caused both outbreaks. There is good evidence that bats are one such natural reservoir, but this remains to be confirmed without doubt.
I hope this response helps!
-EbolaBooze
I imagine they don’t include the outbreaks among animals because that particular table is dealing with the number of humans infected. But, I can’t think of a reason why they wouldn’t include Reston…
So, what would cause it to come back after 10 years? Did people simply not come in contact with the reservoir for that long?
It’s very possible that there wasn’t enough contact, I think. Territorial encroachment into native habitats of different species has only increased in the last few decades, it could be that the most recent spate of outbreaks is due to human-inhabited areas overlapping the habitat of the Ebola reservoir. If we look at the early Ebola outbreaks, every one of those were tracked back to one or a few index cases – indicating a viral reservoir that only has limited contact with humans.
Thank you for your responses! I feel a bit less suspicious now 🙂
No problem at all, I’m always happy to have a good discussion. 🙂